Delirium and Cognitive Impairment
Why is this important?
Cognitive problems including Delirium and Dementia are common in Older Adults presenting to the Emergency Department (ED). Up to 20% of older adults using the ED have some degree of pre-existing cognitive impairment.1 Delirium affects about 10% of older patients in the ED.2 Prolonged stays in the ED are associated with development of delirium in vulnerable people.3
Delirium is associated with a threefold increased mortality rate. It is also associated with accelerated functional decline, accelerated cognitive decline and longer stays in hospital.4,5
It has been shown that over 50% of delirium is missed in the ED and that missed delirium is associated with a three-fold increase in mortality at 3 months.6
How to recognize older adults with delirium or cognitive problems?
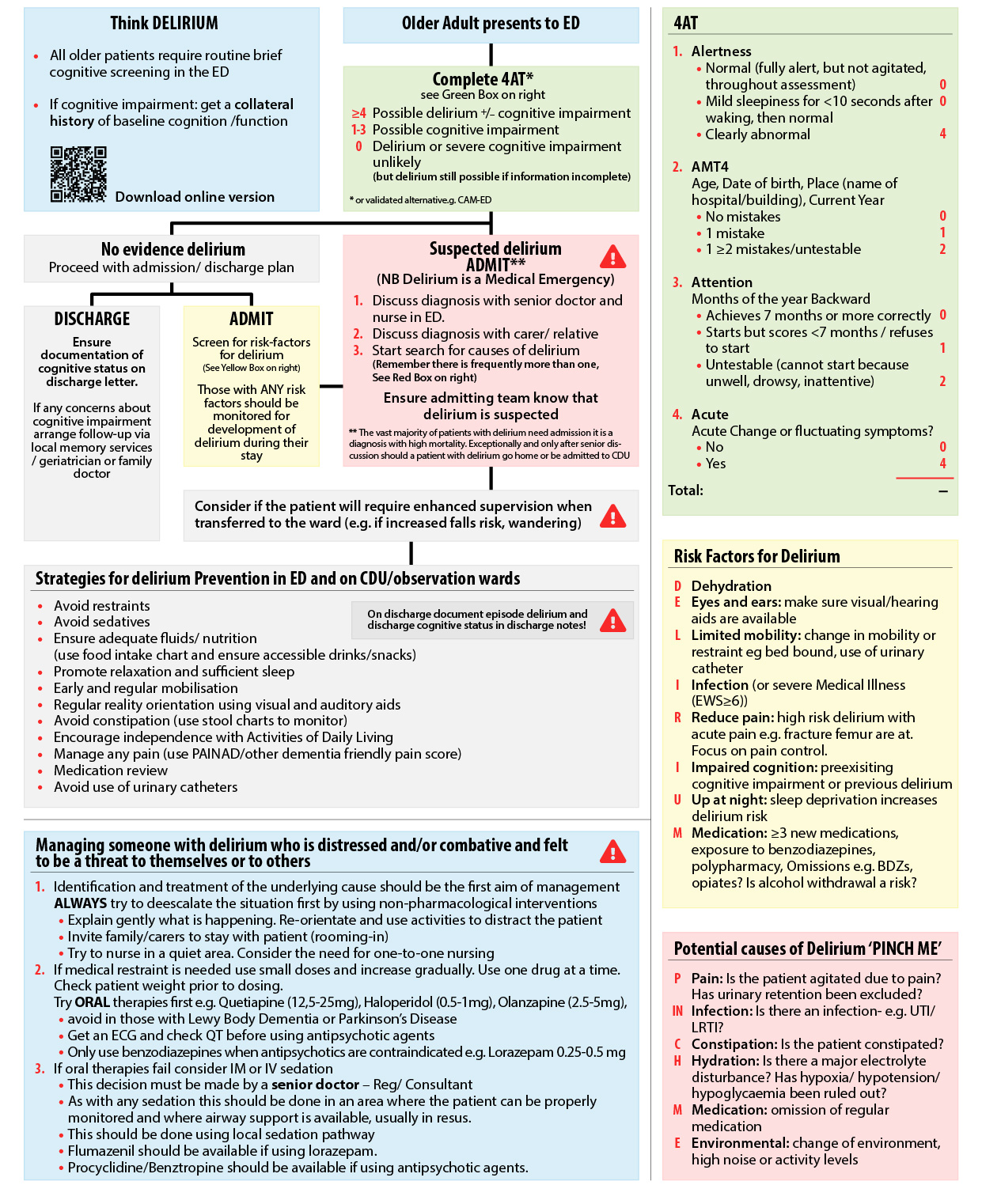
Use a tool to identify those with delirium such as the 4AT7-14 and link this to actions around care such as early review, management in designated spaces, targeted assessment and expedited admission.
What can we do?
- Manage those patients with delirium, or at risk of developing delirium, through multicomponent interventions and regular reorientation. Perform a structured assessment including medications review that aims to identify and reverse potential causes of delirium. Checklists can be used to assist these process.15,16
- Use appropriate aids to assist assessment of pain in older people with cognitive impairment e.g. PAINAD.17
- Where patients have behavioral disturbance or agitation related to cognitive impairment, attempt non-pharmacological treatment methods as first line. 19,20,21,22 Physical restraints should not be used.
- Employ a cautious approach to sedation and only use it when non-pharmacological approaches have failed. Use oral medications in the first instance with the choice of medication tailored to the individual patient. A decision to escalate to IM/IV sedation should be made by a senior doctor and administered in an area where the patient can be properly monitored and where airway support is available, following local and national sedation guidance.
- Link patients who are found to have cognitive impairment in the ED with local structured care pathways for inpatient care, or to their family doctor for further investigation on discharge.21
- Tailor diagnostic investigations for delirium to the individual patient’s history and physical examination findings.
Guideline for identification of cognitive impairment and/or delirium in ED
Toolbox
- Scottish Intercollegiate Guidelines Network Delirium Guideline (SIGN) 2019
- 4AT rapid clinical instrument for delirium detection
- Alzheimer Europe – advocacy agency for European people living with Dementia
- Delirium Pathways in Hospital - Hospital Elder life programme
- Delirium Resources NIDUS – Network for Investigation of Delirium: Unifying Science
Information
This education material was developed by the European Task Force for Geriatric Emergency Medicine, which is a collaboration between the European Society for Emergency Medicine (EUSEM) and the European Geriatric Medicine Society (EuGMS). For more information, please visit: geriEMEurope.eu and follow us on Twitter: @geriEMEurope.
References
- Hustey, Fredric M. et al. The prevalence and documentation of impaired mental status in elderly emergency department patients. Annals of Emergency Medicine, Volume 39, Issue 3, 248 - 253.
- Han J.H., Wilson A., Ely E.W. Delirium in the older emergency department patient: A quiet epidemic. Emerg. Med. Clin. North. Am. 2010;28:611–631. doi: 10.1016/j.emc.2010.03.005.
- Bo M., Bonetto M., Bottignole G., Porrino P., Coppo E., Tibaldi M., Ceci G., Raspo S., Cappa G., Bellelli G. Length of Stay in the Emergency Department and Occurrence of Delirium in Older Medical Patients. J. Am. Geriatr. Soc. 2016;64:1114–1119. doi: 10.1111/jgs.14103.
- Émond M., Grenier D., Morin J., Eagles D., Boucher V., Le Sage N., Mercier É., Voyer P., Lee J.S. Emergency Department Stay Associated Delirium in Older Patients. Can. Geriatr. J. 2017;20:10–14. doi: 10.5770/cgj.20.246.
- Han J.H., Eden S., Shintani A., Morandi A., Schnelle J., Dittus R.S., Storrow A.B., Ely E.W. Delirium in older emergency department patients is an independent predictor of hospital length of stay. Acad. Emerg. Med. 2011;18:451–457. doi: 10.1111/j.1553-2712.2011.01065.x.
- Han J.H., Shintani A., Eden S., Morandi A., Solberg L.M., Schnelle J., Dittus R.S., Storrow A.B., Ely E.W. Delirium in the emergency department: An independent predictor of death within 6 months. Ann. Emerg. Med. 2010;56:244–252.e1. doi: 10.1016/j.annemergmed.2010.03.003.
- O’Sullivan D, Brady N, Manning E, O’Shea E, O’Grady S, O’Regan N, et al. Validation of the 6-Item cognitive impairment test and the 4AT test for combined delirium and dementia screening in older emergency department attendees. Age Ageing 2018;47(1):61-8.
- Bellelli G, Morandi A, Davis DH, Mazzola P, Turco R, Gentile S, Ryan T, Cash H, Guerini F, Torpilliesi T, Del Santo F, Trabucchi M, Annoni G, Maclullich AM. Validation of the 4AT, a new instrument for rapid delirium screening: a study in 234 hospitalised older people. Age Ageing. 2014 Jul; 43(4):496-502.
- Bédard C., Voyer P., Eagles D., Boucher V., Pelletier M., Gouin E., Berthelot S., Daoust R., Laguë A., Gagné A., et al. LO57: Validation of the Ottawa 3DY in community seniors in the ED. CJEM. 2017;19:S47. doi: 10.1017/cem.2017.119.
- Carpenter C.R., Bassett E.R., Fischer G.M., Shirshekan J., Galvin J.E., Morris J.C. Four Sensitive Screening Tools to Detect Cognitive Dysfunction in Geriatric Emergency Department Patients: Brief Alzheimer’s Screen, Short Blessed Test, Ottawa 3DY, and the Caregiver-completed AD8. Acad. Emerg. Med. 2011;18:374–384. doi: 10.1111/j.1553-2712.2011.01040.x.
- Inouye S.K., van Dyck C.H., Alessi C.A., Balkin S., Siegal A.P., Horwitz R.I. Clarifying confusion: The confusion assessment method. A new method for detection of delirium. Ann. Intern. Med. 1990;113:941–948. doi: 10.7326/0003-4819-113-12-941.
- Han J.H., Wilson A., Vasilevskis E.E., Shintani A., Schnelle J.F., Dittus R.S., Graves A.J., Storrow A.B., Shuster J., Ely E.W. Diagnosing delirium in older emergency department patients: Validity and reliability of the delirium triage screen and the brief confusion assessment method. Ann. Emerg. Med. 2013;62:457–465. doi: 10.1016/j.annemergmed.2013.05.003.
- Han, Jin H. et al. A quick and easy delirium assessment for nonphysician research personnel. The American Journal of Emergency Medicine, Volume 34, Issue 6, 1031 - 1036.
- LaMantia MA, Messina FC, Hobgood CD, Miller DK. Screening for delirium in the emergency department: a systematic review. Annals of Emergency Medicine 2014;63(5):551-60.e2.
- Martinez F, Tobar C, Hill N. Preventing delirium: should nonpharmacological, multicomponent interventions be used? A systematic review and meta-analysis of the literature. Age & Ageing 2015;44(2):196-204.
- Siddiqi N, Harrison JK, Clegg A, Teale EA, Young J, Taylor J, et al. Interventions for preventing delirium in hospitalised nonICU patients. Cochrane Database of Systematic Reviews 2016, Issue 3.
- Warden V, Hurley AC, Volicer L. Development and psychometric evaluation of the Pain Assessment in Advanced Dementia (PAINAD) scale. J Am Med Dir Assoc. 2003 Jan-Feb; 4(1):9-15.
- National Clinical Guideline Centre (UK). Delirium: Diagnosis, Prevention and Management. London: Royal College of Physicians (UK); 2010 Jul. (NICE Clinical Guidelines, No. 103.) 12, Treatment of delirium: non-pharmacological (hospital setting) (Accessed 5/9/2019).
- Abraha I., Trotta F., Rimland J.M., Cruz-Jentoft A., Lozano-Montoya I., Soiza R.L., Pierini V., Dessì Fulgheri P., Lattanzio F., O’Mahony D., et al. Efficacy of Non-Pharmacological Interventions to Prevent and Treat Delirium in Older Patients: A Systematic Overview. The SENATOR project ONTOP Series. PLoS ONE. 2015;10 doi: 10.1371/journal.pone.0123090.
- Abraha I., Rimland J.M., Trotta F., Pierini V., Cruz-Jentoft A., Soiza R., O’Mahony D., Cherubini A. Non-Pharmacological Interventions to Prevent or Treat Delirium in Older Patients: Clinical Practice Recommendations The SENATOR-ONTOP Series. J. Nutr. Health Aging. 2016;20:927–936. doi: 10.1007/s12603-016-0719-9.
- Schnitker L, Martin-Khan M, Beattie E, Gray L. What is the evidence to guide best practice for the management of older people with cognitive impairment presenting to emergency departments? A systematic review. Adv Emerg Nurs J. 2013 Apr-Jun;35(2):154-69.
Download
Download the flowchart related to the poster (pdf).